
An Evidence Based Scientific Analysis of Why Masks are Ineffective, Unnecessary, and Harmful PAGE 1 OF 3

An Evidence Based Scientific Analysis of Why Masks are Ineffective, Unnecessary, and Harmful
![]()
PAGE 1 OF 3
About Dr. Meehan
Jim Meehan, MD is an ophthalmologist and preventive medicine specialist with over 20 years of experience and advanced training in immunology, inflammation, and infectious disease. He has performed well over 10,000 surgical procedures. His research experience includes investigating associations between military vaccinations and Gulf War Syndrome. Dr. Meehan is also trained in internal medicine, addiction medicine, endocrinology, integrative medicine, functional medicine, and nutrition.
Dr. Meehan is a former editor of the medical journal, “Ocular Immunology and Inflammation.” Dr. Meehan has peer-reviewed thousands of medical research studies. With this experience and expertise, Dr. Meehan has dedicated his career to protecting his patients and the public from the fraud, corruption, and pseudoscience so often used by agents and agencies whose motives and interests have resulted in American medicine and pharmaceutical drugs becoming the third leading cause of death in the United States.
Key Points
- Decades of the highest-level scientific evidence (meta-analyses of multiple randomized controlled trials) overwhelmingly conclude that medical masks are ineffective at preventing the transmission of respiratory viruses, including SAR-CoV-2.
- Those arguing for masks are relying on low-level evidence (observational retrospective trials and mechanistic theories), none of which are powered to counter the evidence, arguments, and risks of mask mandates.
- The majority of the population is at very low to almost no risk of severe or lethal disease from CoVID-19. Children are at an extraordinarily low risk of dying from CoVID-19. Based on CDC published data, 99.99815% of children that contract CoVID-19 survive.
- Transmission of SARS-CoV-2 among children in schools and daycares is very rare.
- Masks worn properly are well documented to cause harm to their wearers. Masks worn improperly, re-used, or contaminated are dangerous.
- Any reasonable risk to benefit analysis of medical masks concludes that the risks overwhelmingly outweigh the benefits.
- Children are at imminent risk of harm from mask mandates.
Outline
- Evidence Based Medicine: How we (should) make decisions in science and medicine
-
Masks are Ineffective
a. Mixed Messages from the Experts
b. The Evidence Against Masks
c. The Evidence For Masks
-
Masks are Unnecessary
a. Fear and Politics are Subverting Science and Reason
b. Masking Children in Schools is Unnecessary - So Says The Science
- Masks are Harmful: 17 Ways that Masks Can Cause Harm
-
Masking School Children is Ineffective, Unnecessary, and Harmful
a. Mandatory masks in school are a ‘major threat’ to children's’ health, doctors warn
b. Forcing Children to Wear Masks in Schools is Unnecessary
c. Forcing Children to Wear Masks for Long Periods Risks Causing Them Physical Harm
d. Forcing Children to Wear Masks for Long Periods Risks Causing Them Mental and Psychological Harm
Evidence Based Medicine: How we (should) make decisions in science and medicine
High-level versus Low-level Evidence - the Hierarchy of Medical Evidence
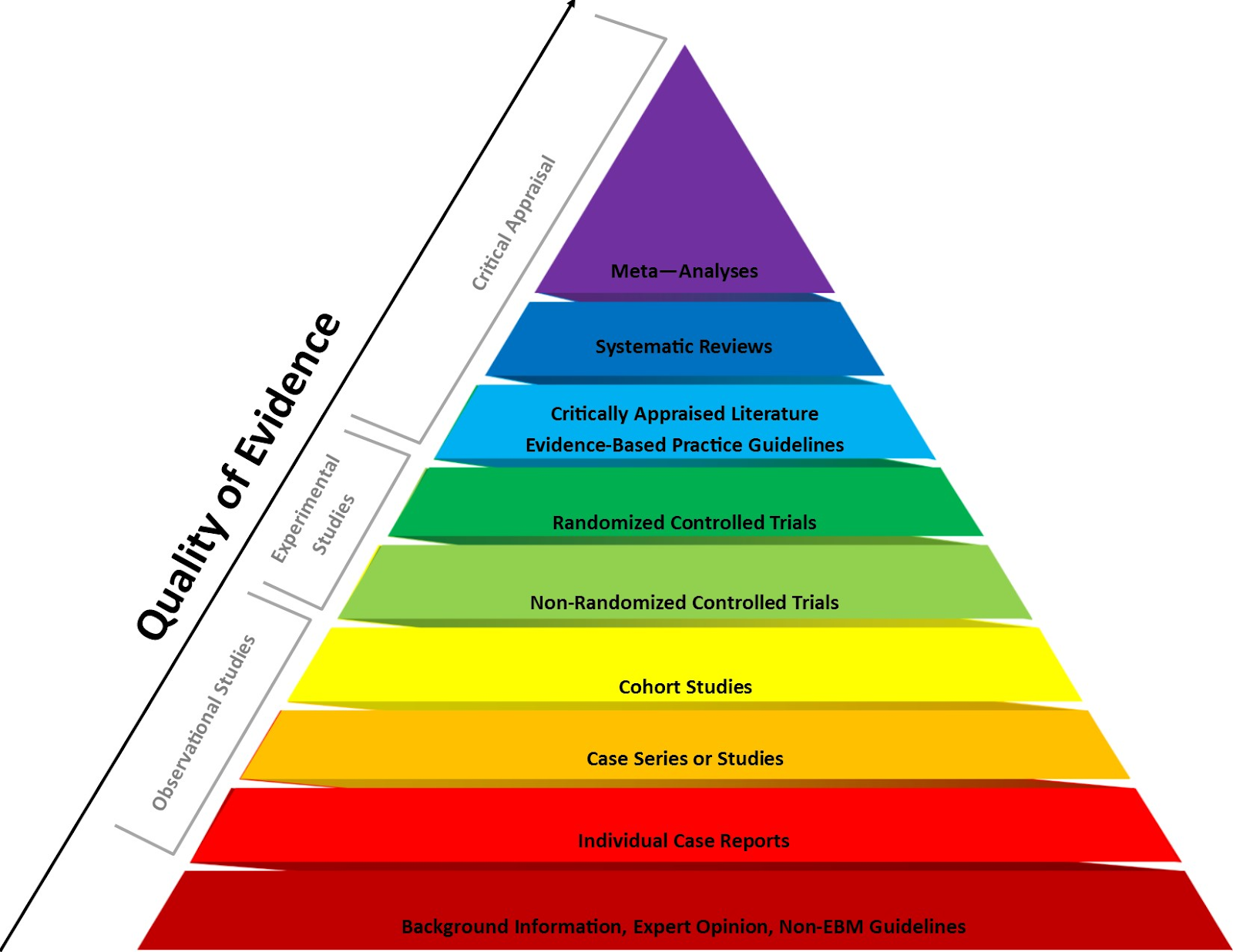
Advocates for mask mandates simply don’t have the highest-levels of scientific evidence to support their arguments. They can only cite low-level science - retrospective observational studies.
Evidence hierarchies are often applied in evidence-based practices and are integral to decision making in medicine and the practice of evidence-based medicine (EBM). The following is from the Wikipedia definition and description of this issue:
A hierarchy of evidence (or levels of evidence) is a heuristic used to rank the relative strength of results obtained from scientific research. There is broad agreement on the relative strength of large-scale, epidemiological studies. More than 80 different hierarchies have been proposed for assessing medical evidence.[1] The design of the study (such as a case report for an individual patient or a blinded randomized controlled trial) and the endpoints measured (such as survival or quality of life) affect the strength of the evidence. In clinical research, the best evidence for treatment efficacy is mainly from meta-analyses of randomized controlled trials (RCTs).[2][3] Typically, systematic reviews of completed, high-quality randomized controlled trials – such as those published by the Cochrane Collaboration – rank as the highest quality of evidence above observational studies, while expert opinion and anecdotal experience are at the bottom level of evidence quality.[2][4]
- Siegfried T (2017-11-13). "Philosophical critique exposes flaws in medical evidence hierarchies". Science News. Retrieved 2018-05-16.
- Shafee, Thomas; Masukume, Gwinyai; Kipersztok, Lisa; Das, Diptanshu; Häggström, Mikael; Heilman, James (28 August 2017). "Evolution of Wikipedia's medical content: past, present and future". Journal of Epidemiology and Community Health. 71 (11): jech–2016–208601. doi:10.1136/jech-2016-208601. ISSN 0143-005X. PMC 5847101. PMID 28847845.
- Straus SE, Richardson WS, Glasziou P, Haynes RB (2005). Evidence-based Medicine: How to Practice and Teach EBM (3rd ed.). Edinburgh: Churchill Livingstone. pp. 102–05. ISBN 978-0443074448.
- Kim Hugel (16 May 2013). "The Journey of Research - Levels of Evidence". Canadian Association of Pharmacy in Oncology. Retrieved 8 December 2019.
Masks are Ineffective
We are all confused by the mixed messages we have received on mask wearing in the community, businesses, and schools. The issue has become tribal, divisive, and for most, confusing. However, I am not confused. I am fully informed on the scientific research related to masks. After reading this, you will be too. Then, you can make the best decisions for you and your family.
As you will learn from the material that follows, the evidence for and against masks should not be confusing. The evidence is clear, masks are ineffective, unnecessary, and harmful.
What's happening in the world today, including the misinformation surrounding community mask wearing, is about political agendas, symbolism, and fear, not science.
Mixed Messages from the Experts:
The CoVID-19 pandemic is about viral transmission. Surgical and cloth masks have repeatedly been shown to offer no benefit in the mitigation of transmission and infection caused by viruses like influenza and SARS-CoV-2. Which is exactly why they have never been recommended for use during the seasonal flu outbreak, epidemics, or previous pandemics.
The failure of the scientific literature to support medical masks for influenza and all other viruses, is also why Fauci, the US Surgeon General, the CDC, WHO, and pretty much every infectious disease expert stated that wearing masks won't prevent transmission of SARS CoV-2. Although the public health "authorities" flipped, flopped, and later changed their recommendations, the science did not change, nor did new science appear that supported the wearing of masks in public. In fact, the most recent systemic analysis once again confirms that masks are ineffective in preventing the transmission of viruses like CoVID-19: https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
If the scientific literature demonstrated that masks were effective, then why, early in the pandemic, did public health experts tell the public not to wear them?
I have heard multiple answers to this question and none of them are reasonable. Here are a couple of the explanations that fail to withstand reasonable scrutiny:
-
Early in the pandemic, Fauci, the CDC, the U.S. Surgeon General, and CDC Director Redfield, all said that masks were ineffective and would not protect the wearer or other members of the public from SARS-CoV-2, the virus that causes CoVID-19. lied to the public and congress about masks being because they were trying to protect the supply of masks for health care workers.
- Early in the pandemic, Fauci, et al, actually told the truth about what years of scientific research overwhelmingly concluded: medical masks don’t work to prevent the transmission or infection of viral respiratory pathogens.
- About a month later, for reasons that appear to have more to do with being lobbied by unnamed interest groups, they all began back-pedaling and claiming that what they said previously was actually a lie, but they lied because they were trying to protect the PPE supply for health care workers.
-
Absolutely NO NEW research appeared to counter the forty years of meta-analyses and systemic reviews of many randomized controlled trials that concluded that masks don’t work to prevent the transmission of upper respiratory viruses.
- Several low-level evidence, retrospective observational, mechanistic studies, and ridiculous “masked hamster cage” studies appeared in the scientific literature.
- The opinions and theories these studies offered were interesting and worthy of consideration, but they failed to explain or counter the large body of prior high-level evidence. In this paper, I will show that none of these observational studies or mechanistic theories countered the large body of high-level evidence built on years of meta-analyzed and systemically reviewed multiple randomized controlled trials
Redfield, Fauci, Birx, the U.S. Surgeon General, the CDC, and the WHO have been terribly inconsistent, confusing, and flip-flopping on masks throughout the pandemic
We were frequently confused by the mixed messages coming from public health agencies. Early in the pandemic Dr. Fauci, the U.S. Surgeon General, and the WHO all told the public, in no uncertain terms, not to wear masks. Then, over the course of the next several weeks and months, the CDC twice changed their recommendations, as did the WHO, and the two agencies' recommendations consistently contradicted each other!
CDC: On June 4, 2020, the CDC published guidance indicating that masks do not deter the spread of Covid-19 after as little as fifteen minutes of exposure to someone with symptoms. CDC, Public Health Guidance for Community-Related Exposure, updated July 31, 2020. https://www.cdc.gov/coronavirus/2019-ncov/php/public-health-recommendations.html
WHO: While recommending the wearing of masks for health professionals, the World Health Organization acknowledged that there is no evidence that mask wearing prevents the spread of Covid-19 and that the science simply does not support requiring otherwise healthy people to wear face masks all day.
“At present, there is no direct evidence (from studies on COVID-19 and in healthy people in the community) on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including COVID-19.” World Health Organization (WHO), Advice on the use of masks in the context of COVID-19, Interim Guidance (June 5, 2020) at 6. https://www.who.int/publications/i/item/advice-on-the-use-of-masks-in-the-community-during-home-care-and-in-healthcare-settings-in-the-context-of-the-novel-coronavirus-(2019-ncov)-outbreak
WHO also acknowledged some of the risks long-term mask use poses to health workers and others:
- self-contamination due to the manipulation of the mask by contaminated hands;
- potential self-contamination that can occur if medical masks are not changed when wet, soiled or damaged;
- possible development of facial skin lesions, irritant dermatitis or worsening acne, when used frequently for long hours
- masks may be uncomfortable to wear;
- false sense of security, leading to potentially less adherence to well recognized preventive measures such as physical distancing and hand hygiene;
- risk of droplet transmission and of splashes to the eyes, if mask wearing is not combined with eye protection;
- disadvantages for or difficulty wearing them by specific vulnerable populations such as those with mental health disorders, developmental disabilities, the deaf and hard of hearing community, and children;
- difficulty wearing them in hot and humid environments.
Public Health Authorities changed their minds, but the science did not change. So, what changed their minds?
More than 40 years of science has consistently concluded that masks don’t work. No new science emerged to counter this conclusion. So, what is the basis for the change in direction that emerged from our public health experts?
The following is the Twitter post from Deborah Cohen, UK correspondent for BBC Newsnight and 2019 British Journalism Award winner, indicates that her investigation of the WHO change from not recommending masks to recommending masks had everything to do with politics and lobbying:
Medically qualified, UK Correspondent @BBCNewsnight | 2019 British Journalism Award winner
“We had been told by various sources WHO committee reviewing the evidence had not backed masks but they recommended them due to political lobbying. This point was put to WHO who did not deny. We said some people think we should not wait for RCTs before putting policies in place”
The ineffectiveness of face masks in stemming the spread of viral respiratory diseases, including Covid-19, is widely known and acknowledged in the scientific and medical literature and scientific communities. Therefore, it seems that the transition in public health recommendations to promote widespread mask mandates was based on a combination of low-level observational studies, speculative mechanistic studies, fear, and, most of all, POLITICS, NOT SCIENCE.
To clear up the confusion, I will argue that the scientific evidence not only does not support the community wearing of face masks, but the evidence shows that healthy people wearing face masks pose serious health risks to wearers.
The Evidence AGAINST Masks
Big Data Analysis of 25 U.S. States and 23 Countries Concludes, “Neither Lockdowns nor Mask Mandates Lead to Reduced COVID Transmission Rates or Deaths”
A new National Bureau of Economic Research (NBER) working paper by Andrew Atkeson, Karen Kopecky, and Tao Zha focused on countries and U.S. states with more than 1,000 COVID deaths as of late July. This analysis is the largest and most comprehensive analysis of the largest datasets to date. In all, the study included 25 U.S. states and 23 countries.
The paper’s conclusion is that the data trends indicate that nonpharmaceutical interventions (NPIs) – such as lockdowns, closures, travel restrictions, stay-home orders, event bans, quarantines, curfews, and mask mandates – do not seem to affect virus transmission rates overall.
Systemic Reviews and Meta-Analysis of Multiple Randomized Controlled Trials Concludes that Face Masks Fail to Prevent Transmission of Viral Respiratory Pathogens
One of the largest and highest level of evidence studies on the effectiveness of face masks on the transmission of respiratory viruses, which was recently released by the CDC, is Jingyi Xiao, et al., Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings— Personal Protective and Environmental Measures, Emerging Infectious Diseases, Vol. 26, No. 5, (May 2020). https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
- This CDC meta-analysis found that face masks failed to provide a significant reduction to virus transmission.
- “In our systematic review, we identified 10 [Randomly Controlled Trials] that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks.”
- There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure.
- Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
Mandates for children to wear face masks fails even a rational basis test, and is clearly not in a child's best interest, when assessed through a factual, evidence-based analysis, rather than a fear-based lens. It is simply not rational to believe that face masks will be properly and studiously worn by young children for up to ten hours in a school day.
In fact, the overwhelming weight of scientific literature to date establishes that face masks do not prevent the spread of COVID-19 by, to, or from, children.
-
Radonovich, L.J. et al., N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial, JAMA. 2019; 322(9): 824–833. doi:10.1001/jama.2019.11645, 2019. https://jamanetwork.com/journals/jama/fullarticle/2749214
- “Among 2862 randomized participants, 2371 completed the study and accounted for 5180 HCW-seasons. … Among outpatient health care personnel, N95 respirators vs medical masks as worn by participants in this trial resulted in no significant difference in the incidence of laboratory-confirmed influenza.”;
-
Long, Y. et al., Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta‐analysis, J Evid Based Med. 2020; 1‐ 9. https://doi.org/10.1111/jebm.12381
- A total of six [Randomized Controlled Trials] involving 9171 participants were included.
- There were no statistically significant differences in preventing laboratory‐confirmed influenza, laboratory‐confirmed respiratory viral infections, laboratory‐confirmed respiratory infection and influenza-like illness using N95 respirators and surgical masks.
- Meta‐analysis indicated a protective effect of N95 respirators against laboratory‐confirmed bacterial colonization.
- The use of N95 respirators compared with surgical masks is not associated with a lower risk of laboratory‐confirmed influenza.
-
See e.g., Patrick Saunders-Hastings, et, al., Effectiveness of personal protective measures in reducing pandemic influenza transmission: A systematic review and meta-analysis, Epidemics, v. 20 (September 2017)
- This systemic review found “face mask use provided a non significant protective effect . . . against 2009 pandemic influenza infection.” https://www.sciencedirect.com/science/article/pii/S1755436516300858
-
An April 2020 review by the Norwich School of Medicine found that “the evidence is not sufficiently strong to support widespread use of face masks”, but supports the use of masks by “particularly vulnerable individuals when in transient higher risk situations.”
- Brainard, et al., face masks and similar barriers to prevent respiratory illness such as COVID-19: A rapid systematic review, April 6, 2020. https://www.medrxiv.org/content/10.1101/2020.04.01.20049528v1
-
Dr. Russell Blaylock, a nationally recognized board-certified neurosurgeon, health practitioner, author, and lecturer warns that not only do face masks fail to protect the healthy from getting sick, but they also create serious health risks to the wearer.
- Dr. Russell Blaylock, Blaylock: Face Masks Pose Serious Risks To The Healthy, Technocracy News & Trends, (posted May 11, 2020). https://www.technocracy.news/blaylock-face-masks-pose-serious-risks-to-the-healthy/
- [Recent studies] found that about a third of the [healthcare] workers developed headaches with use of the mask, most had preexisting headaches that were worsened by the mask wearing, and 60% required pain medications for relief. As to the cause of the headaches, while straps and pressure from the mask could be causative, the bulk of the evidence points toward hypoxia and/or hypercapnia as the cause. That is, a reduction in blood oxygenation (hypoxia) or an elevation in blood C02 (hypercapnia).
- It is known that the N95 mask, if worn for hours, can reduce blood oxygenation as much as 20%, which can lead to a loss of consciousness.
- The importance of these findings is that a drop in oxygen levels (hypoxia) is associated with an impairment in immunity. Studies have shown that hypoxia can inhibit the type of main immune cells used to fight viral infections called the CD4+ T-lymphocyte.
- This occurs because the hypoxia increases the level of a compound called hypoxia inducible factor-1 (HIF-1), which inhibits T-lymphocytes and stimulates a powerful immune inhibitor cell called the Tregs.
- This sets the stage for contracting any infection, including COVID-19 and making the consequences of that infection much graver. In essence, your mask may very well put you at an increased risk of infections and if so, having a much worse outcome. Id.
-
See also Denis G. Rancourt, PhD, Masks Don't Work: A review of science relevant to COVID-19 social policy, Ontario Civil Liberties Association, April 11, 2020. https://www.researchgate.net/publication/340570735
- There have been extensive randomized controlled trial (RCT) studies, and meta-analysis reviews of RCT studies, which all show that masks and respirators do not work to prevent respiratory influenza-like illnesses, or respiratory illnesses believed to be transmitted by droplets and aerosol particles.
- Furthermore, the relevant known physics and biology, which I review, are such that masks and respirators should not work. It would be a paradox if masks and respirators worked, given what we know about viral respiratory diseases: The main transmission path is long residence-time aerosol particles (< 2.5 µm), which are too fine to be blocked, and the minimum-infective-dose is smaller than one aerosol particle.
-
Jacobs, J. L. et al. (2009) Use of surgical face masks to reduce the incidence of the common cold among health care workers in Japan: A randomized controlled trial, American Journal of Infection Control, Volume 37, Issue 5, 417 – 419 https://www.ncbi.nlm.nih.gov/pubmed/19216002
- “N95-masked health-care workers (HCW) were significantly more likely to experience headaches.”
- “Face mask use in HCW was not demonstrated to provide benefit in terms of cold symptoms or getting colds.”
-
Cowling, B. et al., Face masks to prevent transmission of influenza virus: A systematic review, Epidemiology and Infection, 138(4), 449-456. doi:10.1017/S0950268809991658 2010. https://www.cambridge.org/core/journals/epidemiology-and-infection/article/face-masks-to prevent-transmission-of-influenza-virus-a-systematic
- “None of the studies reviewed showed a benefit from wearing a mask, in either [Health Care Workers] or community members in households . . . .”
-
bin-Reza et al., The use of masks and respirators to prevent transmission of influenza: a systematic review of the scientific evidence, Influenza and Other Respiratory Viruses 6(4), 257–267, 2012. https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.1750-2659.2011.00307.x
- “There were 17 eligible studies. … None of the studies established a conclusive relationship between mask ⁄ respirator use and protection against influenza infection.”
-
Offeddu, V. et al., Effectiveness of Masks and Respirators Against Respiratory Infections in Healthcare Workers: A Systematic Review and Meta-Analysis, Clinical Infectious Diseases, Volume 65, Issue 11, 1 December 2017, Pages 1934–1942. https://doi.org/10.1093/cid/cix681
- “Self-reported assessment of clinical outcomes was prone to bias. Evidence of a protective effect of masks or respirators against verified respiratory infection (VRI) was not statistically significant”
In fact, many physicians and researchers now believe that, because the ineffectiveness of face masks in stemming the spread of Covid-19 is so widely known and acknowledged in the scientific and medical communities, the goal of widespread mask mandates is based entirely on low-level observational studies, speculative mechanistic studies, fear, and politics, not science.
-
See Michael Klompas, M.D., M.P.H., et. al., Universal Masking in Hospitals in the Covid-19 Era, New England Journal of Medicine, N Engl J Med 2020; 382:e63 (May 21, 2020). https://www.nejm.org/doi/full/10.1056/NEJMp2006372
- We know that wearing a mask outside health care facilities offers little, if any, protection from infection. . . It is also clear that masks serve symbolic roles. Masks are not only tools, they are also talismans that may help increase health care workers’ perceived sense of safety, well being, and trust in their hospitals. Although such reactions may not be strictly logical, we are all subject to fear and anxiety, especially during times of crisis. One might argue that fear and anxiety are better countered with data and education than with a marginally beneficial mask.
-
See also Lisa M Brosseau, ScD, Margaret Sietsema, PhD, COMMENTARY: Masks-for-all for COVID-19 not based on sound data, Center for Infectious Disease Research and Policy, University of Minnesota, April 1, 2020. https://www.cidrap.umn.edu/news-perspective/2020/04/commentary-masks-all-covid-19-not based-sound-data
- Dr. Brosseau is a national expert on respiratory protection and infectious diseases and professor (retired), University of Illinois at Chicago. Dr. Sietsema is also an expert on respiratory protection and an assistant professor at the University of Illinois at Chicago. They made the following key points in their commentary:
“We do not recommend requiring the general public who do not have symptoms of COVID-19-like illness to routinely wear cloth or surgical masks because:
- There is no scientific evidence they are effective in reducing the risk of SARS-CoV-2 transmission.
- Their use may result in those wearing the masks to relax other distancing efforts because they have a sense of protection.
- We need to preserve the supply of surgical masks for at-risk healthcare workers.
Sweeping mask recommendations—as many have proposed—will not reduce SARS-CoV-2 transmission, as evidenced by the widespread practice of wearing such masks in Hubei province, China, before and during its mass COVID-19 transmission experience earlier this year.
Our review of relevant studies indicates that cloth masks will be ineffective at preventing SARS-CoV-2 transmission, whether worn as source control or as PPE.
Masks as means of “Source Control” - No, My Mask Does Not Protect You From Me
The public is being repeatedly misinformed by catchy (guilt and fear based) marketing messages designed to promote the social responsibility (or guilt) to wear masks as a form of source control: “I wear my mask for you and you wear your mask for me.”
Where is the evidence for these claims? On the websites where these unscientific marketing messages are found, there are never references to science that supports the claims. In fact, despite almost everything that has been drilled into the public psyche regarding masks, has little to know basis in science and absolutely no robust support from the highest-level evidence based research. Masks have never been proven to protect either the wearer or the community from the transmission of respiratory pathogens. Mask mandates during a pandemic are opposed by decades of high level science.
Simply put, the public is being misled by fraudulent claims supported with weak pseudoscience.
The fallacious argument: "Well, if masks don't work, then why do surgeons wear them?"
I'm an ophthalmic surgeon. I specialize in ocular immunology, inflammation, and infectious disease. I’ve performed over 10,000 surgical procedures wearing a surgical mask. I have suffered the detrimental effects that masks caused to my mental and physical function during long surgeries. Because most of the surgeries I performed were microscopic procedures that required fine motor skills, I changed my mask frequently to prevent the detrimental effects of arterial deoxygenation.
However, these facts alone don’t qualify me as an expert on the matter. What qualifies me is my experience as an editor of a medical journal, the fact that I’ve peer-reviewed thousands of pre-print research articles, that I am an expert at reading medical research, distinguishing good science from bad, and separating fact from fiction.
Believe me, the medical literature is filled with bad fiction masquerading as medical science. It is very easy to be deceived by bad science.
Since the beginning of the pandemic I've read hundreds of studies on the science of medical masks. Based on extensive review and analysis, there is no question in my mind that healthy people should not be wearing surgical or cloth masks. Nor should we be recommending universal masking of all members of the population. That recommendation is not supported by the highest level of scientific evidence.
First, the premise that surgeons wearing masks serves as evidence that "masks must work to prevent viral transmission" is a logical fallacy. I would classify this claim as an argument of false equivalence, or comparing "apples to oranges." Surgical masks offer no benefit in protecting patients from the surgeon’s respiratory droplets contaminating the surgical field and the exposed tissues of surgical patients.
Surgeons well-versed in the scientific research regarding medical masks, especially the systemic reviews published by the Cochrane Collaboration Wound Group, know that surgical face masks provide no benefit in the prevention of surgical wound infections.[R][R] Surgeons with experience wearing surgical masks during long surgeries have undoubtedly experienced and understand the detrimental effects masks have on respiration, blood oxygenation, mental, and physical performance. For these science-based reasons, there is a worldwide trend towards surgeons and operating room staff no longer wearing surgical masks during “clean surgery” cases.
Nevertheless, many surgeons continue to wear face masks during clean surgery cases and outpatient minor procedures. We do so more for symbolic purposes, habit, tradition, or, not infrequently, because of institutional ignorance. That is, we are forced to wear masks because it is the ignorant, anti-science policy of the hospital or surgery center where we perform our surgeries.
Although wearing a mask during a clean surgery is unnecessary, there are other surgical cases in which surgical masks, eye protection, and face shields are still a good idea. For example, cases in which bone saws, drills, and other surgical power tools can expose the surgical team to splashes and splatters from the patient’s bodily fluids.
If a surgeon were sick, especially with a viral infection, they would not perform surgery as they know the virus would NOT be stopped by their surgical mask.
Another area of "false equivalence" has to do with the environment in which the masks are worn. The environments in which surgeons wear masks minimize the adverse effects surgical masks have on their wearers.
Unlike the public wearing masks in the community, surgeons work in sterile surgical suites equipped with heavy duty air exchange systems that maintain positive pressures, exchange and filter the room air at a very high level, and increase the oxygen content of the room air. These conditions limit the negative effects of masks on the surgeon and operating room staff. And yet despite these extreme climate control conditions, clinical studies demonstrate the negative effects (lowering arterial oxygen and carbon dioxide rebreathing) of surgical masks on surgeon physiology and performance.
Surgeons and operating room personnel are well trained, experienced, and meticulous about maintaining sterility. We only wear fresh sterile masks. We don the mask in a sterile fashion. We wear the mask for short periods of time and change it out at the first signs of the excessive moisture build up that we know degrades mask effectiveness and increases their negative effects. Surgeons NEVER reuse surgical masks, nor do we ever wear cloth masks.
The public is being told to wear masks for which they have not been trained in the proper techniques. As a result, they are mishandling, frequently touching, and constantly reusing masks in a way that increases contamination and are more likely than not to increase transmission of disease.
Just go watch people at the grocery story or Walmart and tell me what you think about the effectiveness of masks in the community.
If you can't help but believe and trust the weak retrospective observational studies and confused public health "authorities" lying to you about the benefits and completely ignoring the risks of medical masks, then you should at least reject the illogical anti-science recommendation to block only 2 of the 3 ports of entry for viral diseases. Masks only cover the mouth and nose. They do not protect the eyes.
Surgeons and Surgical Masks: Little to No Benefit of Surgical Masks During Surgery
While it may go against “conventional wisdom,” and may seem counterintuitive to those who are not involved in scientific research, the actual scientific evidence does not support the proposition that wearing a mask is an effective method of source control to prevent the spread of infection.
Many surgeons are surprised to learn that when surgical masks are put to the test in randomized controlled trials, they fail to demonstrate benefit. In fact, surgical masks have repeatedly failed to provide evidence of effectiveness as a means of “source control,” even in the one environment where they are so steadfastly adhered to: the operating room. Simply put, based on the actual science face masks have repeatedly been found to be ineffective as a means of source control. Face masks do not protect against the very risk for which the Defendants are forcing small children to wear face masks all day: source control.
-
In 2014, the Cochrane Collaboration “Wounds Group” reviewed all research related to the topic of effectiveness of face masks for preventing surgical wound infections.
- Lipp, A. and Edwards, P., Disposable surgical face masks for preventing surgical wound infection in clean surgery (Review), Cochrane Database of Systematic Reviews 2014, Issue 2. Art. No.: CD002929. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD002929.pub2/epdf/full
- “Three [randomized controlled] trials were included, involving a total of 2113 [surgical team] participants. There was no statistically significant difference in infection rates between the masked and unmasked group in any of the trials.”
-
In 2016, the Cochrane Collaboration “Wounds Group” revisited the topic of effectiveness of face masks for preventing surgical wound infections again in 2016. In this updated review they added any new studies on the topic that entered the literature since their 2014 review (above).
- Vincent, M. & Edwards, P., Disposable surgical face masks for preventing surgical wound infection in clean surgery, Cochrane Database of Systematic Reviews 2016, Issue 4, Art. No.: CD002929. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD002929.pub3/epdf/full
- “Overall, we found very few studies and identified no new trials for this latest update. We analysed a total of 2106 participants from the three studies we found.”
- “All three [randomized controlled trials] showed that wearing a face mask during surgery neither increases nor decreases the number of wound infections occurring after surgery. We conclude that there is no clear evidence that wearing disposable face masks affects the likelihood of wound infections developing after surgery.”
-
See, e.g., Neil W. M. Orr, M.D., Mchir, FRCS, Is a mask necessary in the operating theatre?, Annals of the Royal College of Surgeons of England, vol. 63, 1981. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2493952/pdf/annrcse01509-0009.pdf
- This six month long study showed a significant decrease in the rate of patient infections when masks were NOT worn in an operating theater.
-
Ritter, MA, et al., The operating room environment as affected by people and the surgical face mask. Clinical Orthopaedics and Related Research: September 1975 - Volume 111 - Issue - p 147-150. https://journals.lww.com/clinorthop/Citation/1975/09000/The_Operating_Room_Environment\_as _ Affected_by.20.aspx
- “The wearing of a surgical face mask had no effect upon the overall operating room environmental contamination...”
-
Da Zhou et al., Unmasking the surgeons: the evidence base behind the use of face masks in surgery, Journal of the Royal Society of Medicine; 2015, Vol. 108(6) 223–228. https://journals.sagepub.com/doi/pdf/10.1177/0141076815583167
- The paper analyzed numerous studies.
- The use of surgical face masks is ubiquitous in surgical practice. Face Masks have long been thought to confer protection to the patient from wound infection and contamination from the operating surgeon and other members of the surgical staff... However, overall there is a lack of substantial evidence to support claims that face masks protect either patient or surgeon from infectious contamination. (emphasis added)
- Zahid Mehmood Bahli, Does evidence based medicine support the effectiveness of surgical face masks in preventing postoperative wound infections in elective surgery?, J Ayub Med Coll Abbottabad 2009; 21(2). http://www.ayubmed.edu.pk/JAMC/PAST/21-2/Zahid.pdf
-
- “No significant difference in the incidence of postoperative wound infection was observed between masks group and groups operated with no masks. There was no increase in infection rate in 1980 when masks were discarded. In fact there was a significant decrease in infection rate.” (emphasis added)
-
Ana E. Figueiredo, et. al., Bag Exchange in Continuous Ambulatory Peritoneal Dialysis Without Use of a Face Mask: Experience of Five Years, Renal Unit, Hospital São Lucas, Porto Alegre, Brazil. http://www.advancesinpd.com/adv01/21Figueiredo.htm
- “Peritonitis rates reported during our observation period are compatible with those seen in other centers and support the hypothesis that routine use of a face mask during CAPD bag exchange may be unnecessary.”
-
M.W. Skinner, B.A Sutton, Do Anaesthetists Need to Wear Surgical Masks in the Operating Theatre? A Literature Review with Evidence-Based Recommendations, Anaesthesia and Intensive Care, Vol. 29, No. 4, August 2001. https://journals.sagepub.com/doi/pdf/10.1177/0310057X0102900402
- The evidence for discontinuing the use of surgical face masks would appear to be stronger than the evidence available to support their continued use. . . .
- There is little evidence to suggest that the wearing of surgical face masks by staff in the operating theatre decreases postoperative wound infections.
- Published evidence indicates that postoperative wound infection rates are not significantly different in unmasked versus masked theatre staff.
- However, there is evidence indicating a significant reduction in postoperative wound infection rates when theatre staff are unmasked.
- Currently there is no evidence that removing masks presents any additional hazard to the patient. (emphasis added).
-
See Eva Sellden, M.D., Ph.D., Is Routine Use of a Face Mask Necessary in the Operating Room?, Anesthesiology 2010; 113:1447, the American Society of Anesthesiologists, Inc. https://pubs.asahq.org/anesthesiology/article/113/6/1447/9572/Is-Routine-Use-of-a-Face-Mask Necessary-in-the
- “Our decision to no longer require routine surgical masks for personnel not scrubbed for surgery is a departure from common practice. But the evidence to support this practice does not exist . . . .”
Cloth Masks are Ineffective and May Increase the Risk of Transmission
Cloth masks are absolutely ineffective. Worst yet, they may increase the incidence of disease in wearers and the population.
Despite the high-level scientific evidence against cloth masks, the CDC made the inexcusable mistake of telling us cloth masks worked. They even provided directions on their website for making homemade cloth masks.
A July 2020 review by the University of Oxford, Centre for Evidence-Based Medicine found that there is no evidence that cloth masks are at all effective against virus infection or transmission.
- Jefferson, Tom & Heneghan, Carl, Masking lack of evidence with politics, Centre for Evidence-Based Medicine, July 23, 2020. https://www.cebm.net/covid-19/masking-lack-of-evidence-with-politics/
A July 2020 study by Japanese researchers found that cloth masks “offer zero protection against coronavirus.”
-
Naoya Kon, Cloth face masks offer zero shield against virus, a study shows, The Asahi Shimbun, study by Kazunari Onishi. http://www.asahi.com/ajw/articles/13523664
- “This experiment reconfirmed that wearing cloth and gauze masks can’t prevent virus infection.”
In an August 2020 article, Denis G. Rancourt, PhD, a Researcher, Ontario Civil Liberties Association, debunks supposed “studies” purporting to support compelled face mask use for the general population.
-
See Rancourt, Face masks, lies, damn lies, and public health officials: “A growing body of evidence” August 2020. https://www.researchgate.net/publication/343399832_Face_masks_lies_damn_lies_and_public_hea lthofficialsAgrowingbodyofevidence
- “[T]here is no policy-grade evidence to support forced masking on the general population, . . . all the latest-decade’s policy-grade evidence points to the opposite: NOT recommending forced masking of the general population.”);
- No [randomized controlled trial] study with verified outcome shows a benefit for [health-care workers] or community members in households to wearing a mask or respirator. There is no such study. There are no exceptions. Likewise, no study exists that shows a benefit from a broad policy to wear masks in public (more on this below).
- Furthermore, if there were any benefit to wearing a mask, because of the blocking power against droplets and aerosol particles, then there should be more benefit from wearing a respirator (N95) compared to a surgical mask, yet several large meta-analyses, and all the RCT, prove that there is no such relative benefit.
- Masks and respirators do not work. (emphasis added);
- Denis G. Rancourt, PhD, Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy, River Cities Reader, June 11, 2020. https://www.rcreader.com/commentary/masks-dont-work-covid-a-review-of-science-relevant-to covide-19-social-policy
- see also, Todd McGreevy, Still No Conclusive Evidence Justifying Mandatory Masks, River Cities Reader, August 12, 2020. https://www.rcreader.com/commentary/still-no-conclusive-evidence-justifying-mandatory-masks
I presented a partial list of the various meta-analyses and systemic reviews of multiple randomized controlled trials (RCTs). The studies represent the highest level of evidence that masks don’t work.
This WHO commissioned study is the best counter to my arguments. To any trained researcher, this study falls far short of countering decades of the science previously presented.
Advocates for mask mandates simply don’t have the highest-levels of scientific evidence to support their arguments. They can only cite low-level science - retrospective observational studies. The WHO study is a cleverly disguised example of low-level garbage dressed up to appear better than what it is. You have to examine the details to detect the weak deception.
The Evidence FOR Masks
PAGE 1 OF 3


i Witness NEWS
The Truth Never Suffers from Honest Examination!
PUBLIC DISCLOSURE - Things Hidden
Archives
Tag cloud
Related blogs

An Evidence Based Scientific Analysis of Why Masks are Ineffective, Unnecessary, and Harmful PAGE 2 0F 3
Scientists all over the world are raising...An Evidence Based Scientific Analysis of Why Masks are Ineffective, Unnecessary, and Harmful PAGE 3 OF 3
Furthermore, these risks are compounded by the...